Idiopathic scoliosis
Background
Scoliosis is a complex spinal disease characterized by an abnormal curvature. Adolescent Idiopathic Scoliosis (AIS) is a lateral C or S curvature that begins at the peak of adolescent growth [1]. The global prevalence of scoliosis is 0.47%-5.2%, and the male-to-female ratio ranges from 1.5:1 to 3:1 and increases significantly with age, which is highly harmful to the physical and mental health of adolescents [2]. According to the severity classification, it can be divided into four categories: 1. Cobb angle 10° is the normal spine range. 2.10°40° for severe scoliosis. AIS can be progressive or stable, where the severity of scoliosis increases before or after the completion of bone development [3]. Today’s treatment methods are diverse, but it is not clear which therapy is the best, mainly divided into conservative treatment and surgical treatment. Support therapy accounts for the main body of conservative treatment. Studies have also recommended massage as a supplement and alternative to treat patients with idiopathic scoliosis [4]. In recent years, specific exercise therapy has gradually emerged, among which is Schross exercise therapy (Schroth Method), which is one of the representative programs.
The Schroth method is a new hope for patients with scoliosis. The correction method was developed by German physical therapist Katharina Schroth in the early 20th century, incorporating biomechanics, postural correction, and patient self-management. It was later further developed by her daughter Christa and promoted in academia by her grandson, a private orthopedic surgeon [5]. As a non-invasive approach, it has gained general recognition for its efficacy in controlling scoliosis progression and improving patient quality of life.
Katharina Schroth The journey of developing her approach is very personal. She was herself diagnosed with scoliosis and began to seek a non-surgical solution to relieve her symptoms. Drawing on her dance background, she began to experiment with posture and movement techniques and eventually developed a systematic approach to solving scoliosis. Katharina, working with her physiotherapist daughter Christa Lehnert-Schroth, has perfected her approach after decades of research and clinical practice. Their work laid the foundation for what is now called the Schroth method, which has since evolved through continued research and progress in the field of physical therapy.
Modern core ideas and implementation methods of Schroath therapy
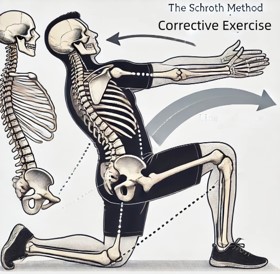
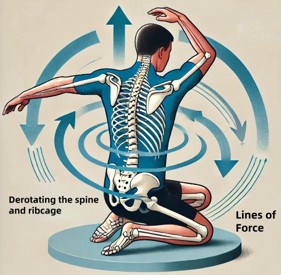
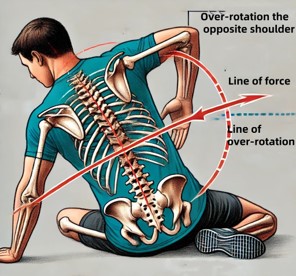
Theory: The core of Schroth’s therapy is to understand scoliosis as a complex three-dimensional deformity of the spine. The founders did not see scoliosis as mere scoliosis but recognized the rotation and asymmetry of scoliosis. This insight led it to develop corrective training designed to combat these multidimensional malformations. Furthermore, Schroth Methods recognizes the role of postural imbalance, muscle asymmetry, and breathing patterns in exacerbating scoliosis. By addressing these triggers, the therapist aims to restore postural balance and enhance spinal alignment. The approach also draws on the principle of neuroplasticity, emphasizing the brain’s ability to tailor and reorganize neural pathways according to targeted exercise interventions.
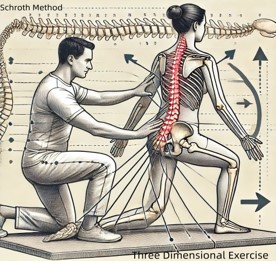
Implementation approach: The implementation of Schroth therapy involves a systematic approach tailored to the unique characteristics of each scoliosis patient. This process usually begins with a comprehensive assessment assessing spinal curvature, muscle imbalance, and functional limitations. Based on these assessments, the therapist designed personalized treatment options, including specific exercises and breathing techniques. The program is based on sensorimotor and kinematic principles, including corrective exercises, postural self-correction, breathing skills, education, and home practice. By using a mirror, patients learn to visually see their deformity and thus self-correct the wrong posture. The unique pull of Schroth therapy is essential for postural correction, while rotational breathing is the cornerstone of Schroth methods [5,6].
Schroth Designed to restore postural balance, reduce spinal stress, and improve neuromuscular control, and therapy, following several basic principles [7], These principles include:
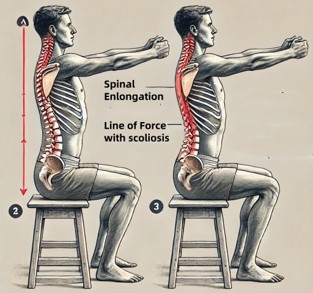
Three-dimensional approach: Unlike traditional therapies, which focus only on spinal curvature, the Schross method uses a holistic perspective to solve the three-dimensional properties of scoliosis. By combining specific exercises and breathing techniques, it aims to elongate the spine, correct rotational deformity, and rebalance muscle asymmetries.
Individualized treatment: The Schroth approach recognizes the unique biomechanical features of each patient’s scoliosis and emphasizes personalized treatment planning. The therapist evaluates the patients’ spinal curvature, muscle imbalance, and functional limitations to tailor the exercise to their specific needs.
Rotational breathing: At the core of Schroth’s method is the concept of rotary breathing, which uses conscious inspiration and expiration to promote spinal elongation and muscle relaxation. By coordinating breathing patterns with corrective movements, patients learn to optimize thoracic expansion and improve postural alignment.
Correction exercises: Through a series of specialized exercises, guide the patient to actively exercise the muscles and retrain the exercise patterns to counteract scoliosis. These exercises may involve elongation, stabilization, and reinforcement techniques, often using props such as therapeutic balls, resistance bands, and Schross sticks [8].
Biomechanical analysis of Schroth therapy
Spine bending management: The Schroth method utilizes a detailed assessment of the patient’s spine bending patterns, usually including measuring the Cobb angles and determining the vertex of the curvature. This evaluation helps to design specific exercises to reduce the magnitude and rotation of the curves. This approach addresses both primary and secondary (compensatory) spinal curvature and focuses on elongation, abduction, and stabilization of the spine.
Rib dynamics: This method carefully examines the relationship between ribs and scoliosis, especially focusing on rib hump deformity and rib asymmetry. The purpose of the exercise is to promote the motion of ribs, correct thoracic deformity, and promote the improvement of lung function and uniform distribution of thoracic. Compliance breathing exercises are a key component that encourages patients to expand the concave surface of the thorax, thereby reducing rib protrusion and enhancing thoracic symmetry [15]. Schroth The breathing technique, also known as “rotational breathing,” aims to prolong the trunk and correct spinal imbalances. The primary goal is to improve patient posture and spine alignment by using clinicians to maintain correct posture and utilize repetitive exercises. Use a mirror, and the patient is taught to imagine the collapsed area where he/she needs to extend or contract [51].
Load distribution: Scoliosis leads to load asymmetry in the vertebral body and the intervertebral disc. The Schroth training method aims to redistribute these loads through specific exercises for spinal extension and abduction. By addressing the problem of muscle imbalance and promoting more spinal neutrality, the method helps to reduce the abnormal mechanical pressure imposed by the spine and its associated structures, with the potential to slow the progression of spinal curvature. Vanja Dimitrijevic and Tijana Scepanovic et al suggest that tension unique to Schroth therapy is crucial for postural correction [54].
Movement chain: This method takes into account the whole motion chain, including the spine, pelvis, and lower limbs. It recognizes that scoliosis causes pelvic tilt and inconsistent leg lengths, which further aggravates spinal curvature. Practice in the Schroth training method involves pelvic correction aimed to achieve balanced activation of muscles throughout the body, thus supporting the overall biomechanical arrangement and function [50]. Schroth Methods Teach physiotherapists to first strengthen and correct pelvic alignment exercises, followed by spinal elongation, torsion, and stabilization [53]. The whole correction process is mainly completed by axial lengthening, asymmetric sagittal plane straightening, rotating breathing, and developing frontal plane straightening and muscle activation [51].
Neuromuscular re-education: This method emphasizes neuromuscular re-education to enhance proprioception and body awareness. Through persistent practice, patients learn to recognize and maintain correct posture, thus reducing the curve trend. This is particularly important for long-term treatment because it allows patients to actively participate in treatment and maintain spinal corrective posture in daily life [15].
Effectiveness of Schross therapy in patients with AIS
Improve the somatic function
Recent studies have confirmed that Schroth methods can effectively improve the symptoms and signs of AIS. Deniz Aktan and Yıldız Erdoganoglu conducted a 7-day Schroth intervention study in patients with AIS and found that even short-term correction improved important physical indicators, including symptoms and signs. Such as trunk rotation angle (Angle of trunk rotation, ATR), trunk muscle endurance, dynamic balance, and health-related quality of life [9]. Karina Zapata et al. performed Schroth correction in a patient with combined lumbar scoliosis and examination at 1 week and 1 year and found that the initial effect of main curvature-lumbar Cobb angle was not obvious, but improved significantly after one year of active correction exercise. It was believed that the improvement of exercise ability and spinal flexibility led to the improvement of the Cobb angle [10].
Improve the imaging index
Gao Ang and Li Junyu et al. agree that Schroth can delay the curve progression during the intervention. However, patients need to meet the “Risser sign at 3-5 and Cobb angles at 20°-40°”. After corrective training, cervical alignment and shoulder balance also improved significantly [11]. The Jaeyong Park and Wi-Young So studies opposed and argued that Schroth motion correction allowed clear positive changes in Cobb angles, scoliosis meter readings, lumbar lordosis, and calf valgus angles, regardless of severe scoliosis. It should be clinically recommended to patients along with “wearing other aids” [12].
Kira Skaggs and Adrian J. The retrospective study by Lin et al only allowed patients to stand in the Schroth training position. Compared with the normal standing position, the X tablets showed significant improvement in the Cobb angle of the main curve. The leg length of both pairs was measured, and the difference was also significant [13]. Nikos K Aravidas and Paris I Akovidis et al. agree that the (Physiotherapeutic scoliosis-specific exercise, PSSE-Schroth) method is effective for AIS around the most dangerous developmental phase of early growth, in patients with lateral degrees <25°. In particular, this method reduces the chance of requiring braces, which is more advantageous than general or non-specific exercise [14].
Improve the overall function
Tugba Kuru and I pek Yeldan et al. showed that Schroth performed under clinic guidance is superior to exercise programs performed only at home, with results indicating significant improvements in Cobb angle, quality of life, and trunk rotation [15]. Gao A and Li JY et al. found that Schroth improved health-related quality of life in AIS patients with Risser signs between 3-5 and Cobb angles between 20° and 40° (Health-Related Quality-of-Life, HRQoL), with no progression of curvature during follow-up and an improvement in cervical and shoulder alignment [11].
A systematic review and meta-analysis of exercise therapy
Faris Khan and Lucy Chinnery et al. noted that corrective exercise therapy is more effective than standard physical therapy in reducing the scoliosis curve of patients with Idiopathic Scoliosis (IS); and that any type of “correction-based exercise” is more comfortable than support therapy without reducing the effect of nonsurgical treatment [16]. The study of Fan Yunli and Ren Qing et al pointed out that “ there is moderate quality evidence to support that specific scoliosis movement (Scoliosis Specific Exercise, SSE) can significantly reduce Cobb angles and improve trunk asymmetry, but the effect of brace + SSE on the treatment of moderate scoliosis is unclear, and there is insufficient evidence that SSE has any effect on changes in quality of life (Quality of Life, QoL) [17].” Meng-Jia You and Ze-Yu Lu et al. suggested that the effect of PSSE is not affected by the duration and type of intervention, but may be influenced by the initial Cobb angle. The quality of the supporting evidence was low to moderate [52].
Hagit Berdishevsky and Victoria Ashley Lebel et al. the modern modification of patients with Early Onset Scoliosis (EOS) and adults. Sagittal deformities, such as hyperkyphosis (Scheuermann’s kyphosis) and lordosis (rounded back), can also be treated with Schroth practice. Juvenile idiopathic scoliosis (Juvenile idiopathic scoliosis, JIS) is also treated with a less intensive modified Schroth therapy. The treatment of AIS is to prevent curve development before the end of development. Adult scoliosis is treated with a modified Schrotter method based on the severity of pain, the degree of spinal deformity, and stiffness [18]. They agree on the effectiveness of PSSE-Schroth in the treatment of scoliosis, but it is unclear which methods and exercises are most effective for patients, and further research is needed. Similarly, Vaiva Seleviciene and Aiste Cesnaviciute et al. [19], J Bettany-Saltikov, and E Parent et al. [20], all the articles support that PSSE is better than mainstream brace therapy. However, there is still a lack of evidence to prove which exercise correction method is the most effective, and more high-quality research and effective evidence are needed in the future. J.Y. Thompson and E.M. Williamson et al. also suggested that SSE may be effective in improving spinal deformities in patients with AIS, but the quality of evidence is low. Therefore, future studies should adopt rigorous methods and reporting standards to evaluate the relevant clinical indicators and cost-effectiveness [49].
Based on the status of these studies, Jie Xu and Meng Chen et al. noted that there are not many studies comparing the clinical efficacy of various non-surgical therapies in recent years and that these studies could not be directly compared due to differences in inclusion eligibility criteria and outcome measures. Meanwhile, the existing growth potential and progression risk assessment system are inconsistent, further affecting clinical efficacy studies. It is recommended that the patient treatment effect (such as appearance, disability, pain, and quality of life) be the core, and the main evaluation criteria for scoliosis progression should be standardized [21]. Meanwhile, Anthony N. Baumann and Kevin Orellana et al noted that PSSE may not be able to provide clinically significant improvement in AIS and Cobb angle in patients compared to control intervention. It is unclear whether the improvement in PSSE remains after 2 years or simply delayed natural history [56]. At present, there are many research articles on AIS of exercise therapy intervention, and the correction effect of this disease has been confirmed. Schroth Methods There are few systematic reviews on AIS, and this review is the first summary, so it has innovative significance in promoting deep Schroth research.
Synergy of combining other therapies
Schroth combining other exercise therapies RRECAJ-MALAJ S and BEQAJ S et al. A 24-week Schroth and Pilates (Pilates) intervention combining Schroth and Pilates practice in AIS patients with mild and moderate scoliosis was statistically significant in reducing Cobb angle and ATR, improving chest expansion and trunk flexion, and improving quality of life [22].
Schroth combined with brace Fang Mingqiao and Huang Xiaoli et al. found that the Schroth method can improve the flat back abnormality caused by the brace, and the combination of the Chêneau brace and Schroth method can improve the coronal balance of patients better than using the brace alone. At the same time, adding the Schroth method can improve HR-QoL for AIS patients [23]. Yasin Larni and Holakoo Mohsenifar et al used the Boston brace combined with the Schroth method to confirm the conclusion of the above study [24].
Moreover, Kemal Kurak and ABdullahal Al Tunhan et al. added the muscle Electrical Stimulation (EMS) on the basis of Schroth and found that sports corrective exercise can shorten the recovery time of adolescent patients, which is also beneficial for the rapid recovery of athletes after injury. The improvements for the Cobb angle and QoL were also increased [25].
Tuğba Kuru Çolak and Burcin Akcay et al. intervened using the Schroth latest protocol combined with a Cheneau-type brace and found that good and regular communication with patients and family could improve adherence to treatment. AIS patients receiving exercise and stent combination had increased adherence with significantly improved Cobb angle and ATR and sustained outcomes compared to other patients receiving only one of the treatments [26].
Schroth combines nursing Sanja Schreiber and Eric C. Parent et al. added Schroth to a standard of care for a 6-month intervention and found that the severity of the scoliosis angle was significantly lower than in patients observing or using a brace alone. This protocol rigorously demonstrates the short-term benefits of the Schroeter PSSE for AIS [27]. Similarly, Nada Mohamed and Vivechana Acharya et al. added Schroth therapy with standardized care (observation or brace) to effectively reduce the asymmetry measurement value in the back of AIS patients. In terms of treatment intention and protocol statistics, the effect was similar, but the quantitative asymmetry measurement of patients combined the Schroth in the use of nursing, and the patients improved more significantly [28].
In conclusion, the utility of Schroth-specific scoliosis gymnastics therapy (SSE) as an effective treatment is strengthened by a variety of comprehensive treatment options. A combination of other therapies, such as bracing, pilates practice, or standard of care measures, can not only accelerate the rehabilitation process, but also provide better treatment results in correcting spinal deformities, improving physiological function, and improving the patient’s quality of life. This suggests that treatment strategies for idiopathic scoliosis should favor a comprehensive approach that combines Schroth therapy with other adjuvant therapies to achieve optimal treatment outcomes.
Table 1: Effectiveness of Schroth therapy in patients with AIS.
| Author and years of publication |
Evaluation of the content |
Effect |
Other things need to be explained |
| Deniz Aktan (2021) |
ATR, postural recovery, trunk muscle endurance, flexibility, dynamic balance, body image, perception of cosmetic deformity, HR-QoL |
Imaging parameters: ATR↓ *, postural symmetry ratio ↑*, trunk muscle endurance ↑*, dynamic balance scores ↑* cosmetic deformity perception ↓*, HR-QoL ↑* |
|
| Karina Zapata (2016) |
Lumbar major curvature and thoracic lateral curvature |
after training; main Cobb↓*, compensatory Cobb↑ |
Future analysis should be done to research the time that is needed when combined with wearable technology |
| Ang Gao (2021) |
HRQOL, Overall CVA and SVA, C2-C7 Cobb angle, C2-7 SVA, LL, TK, TLK, CHD, Cla -A T1 tilt |
HRQOL: VAS↓, SRS-22 (Pain ↓*, self-image ↑*) Imaging: Overall Cobb angle↓, SVA↓, CVA↓, Cobb angle of C2-C7↓, TK↓, TLK↓, and LL↓, CHD↑ and Cla-A↓, SVA of C2-C7↓*, T1 tilt ↓* |
|
| Jaeyong Park (2022) |
Cobb angle, scoliometer, LL, calcaneal valgus angle |
Cobb angle↓, Scoliometer reading↓, Lumbar Lordosis↓*, Left Calcaneal Valgus Angle↓*, right Calcaneal Valgus↓* |
|
| Kira Skaggs (2020) |
Main Cobb angle, compensatory curve, coronal balance, shoulder balance, mean leg length discrepancy |
Main Cobb angle ↓*, compensatory curve ↓*, coronal balance ↑ and shoulder balance ↑, Mean leg length discrepancy ↓* |
|
| Nikos Karavidas (2024) |
Cobb angle, Number of patients who required a stent at skeletal maturity, SRS-22 questionnaire, TAPS questionnaire, ATR, TRACE scale Curve ↓*, Cobb in thoracic ↓, Cobb in lumbar ↓*, ATR ↓* most SRS-22 scores improved *, except Pain and Function scores TAPS scores ↑*, TRACE scores ↓* |
Curve ↓*, Cobb in thoracic ↓, Cobb in lumbar ↓*, ATR ↓* most SRS-22 scores improved *, except Pain and Function scores TAPS scores ↑*, TRACE scores ↓* |
|
| Tuğba Kuru (2016) |
Cobb angle, ATR, waist asymmetry, maximum hump height, SRS -23 |
Cobb angle ↓*, ATR ↓*, height of hump↓, waist asymmetry↓ *, SRS-23 total scores↑ |
|
Note: ATR: Angle of Trunk Rotation; HR-QoL: Health-Related Quality of Life; SRS-22: SRS-22 Patient Questionnaire; CVA: Coronal Vertical Axis;
SVA: Sagittal Vertical Axis; LL: Lumbar Lordosis; TK: Thoracic Kyphosis; TLK: Thoracolumbar Kyphosis; CHD: Coracoid Height Difference; Cla-A:
Clavicular Angle, TAPS: Trunk Appearance Perception Scale; SRS-23: Scoliosis Research Society-23 Questionnaire; ↑: Increase, ↓: Decrease
*: Significant Difference
Table 2: The effects of correcting AIS Schroth in combination with other therapies.
| Author and date of publication |
Joint content |
treatment effect |
replenish |
| Shkurta Rrecaj -Malaj (2020) |
Pilates |
Cobb ↓* ATR↓* chest expansion↑* trunk flexion*↓ QoL↑* |
|
| Ming-Qiao Fang (2022) |
Chêneau brace |
Cobb↓*, C7-CSVL↓*, TK↓*, SVA, LL, PT, SS, and PI all improved HR-QoL↑* Improve the flat back |
|
| Yasin Larni (2022) |
Boston Brace |
postural control: both OE/CE COPr ↓*, COPv ↓* COPsa ↓* ATR ↓* |
|
| Kemal Kurak (2022) |
EMS |
In EMSS and CG Cobb angle↓*, EMSS SRS-22 scale scores ↑*, SE SRS-22 scale scores ↑*, except pain worsen |
SE Cobb angle ↓ |
| Tuğba Kuru Çolak, (2023) |
Chêneau -Type Brace |
Cobb↓* ATR ↓* |
Average height↑ higher than baseline at the final return visit. |
| Sanja Schreiber (2016) |
Standard of Care |
ITT analysis:1. Largest Cobb angle↓*, sum of curves↓*(6 months).
Covariates: weight and classifications 3cp and 4cp had main effects on the Largest Curve*.
Weight and classification 3cp had significant main effects on the Sum of Curves Per person analysis: Largest Cobb angle↓*, sum of curves↓* |
|
| Nada Mohamed (2024) |
Standard care |
Group* time: Combined: 1. ITT analysis, 6 months RMS↓* Per-protocol analysis:RMS ↓* MaxDev
↓*. Control: In the last 6 months RMS and MaxDev have shown no difference. |
|
Note: COPr: The COP Range; COPv: COP Velocity; COPsa: COP Sway Area; OE: Open Eyes; CE: Close Eyes; ATR: Angle of Trunk Rotation;
EMSS: EMS Schroth Exercise Group; SE: Schroth Exercise Group; CG: Control Group; ↑: Increase; ↓: Decrease; *: Great Significance.
Supplements: 1. For every 1 kg increase in weight, patients had on average 0.44° larger Largest Curve. 2. patients classified as 3cp and 4cp had on
average 12.1°and 8.3° (larger Largest Curve than patients classified as 3c, respectively. 3. the heavier patients and patients classified with the 3cp
curve type had on average the largest Sum of Curves. 2. Age had a significant main effect for both MaxDev and RMS Patients classified as 4C curve
types had better RMS and MaxDev compared to those classified as 3C. Similarly, patients classified as 4CP, had better RMS and MaxDev compared to
those classified as 3CP 3. more significant decrease in quantitative asymmetry measurements.
Comparative advantages of Schross therapy and other conservative therapies and surgical treatments
Jalpa Shah, T Padma Priya showed The Schroth and Scoliosis Scientific Training Method (Scientific exercise approach to scoliosis, SEAS) approach has improved Cobb angle in patients with mild to moderate AIS. In contrast, the Schroth regimen showed greater improvement than the SEAS [29]. R.A. Mohamed and A.M. Yousef used the ontological neuromuscular promotion technique (Proprioceptive neuromuscular facilitation, PNF) mode and Schroth to intervene in the right-curved female students aged 14-16 years, respectively, and found that PNF could not produce a significant improvement in ATR. While ATR is an important indicator for evaluating efficacy, the use of these PNF modalities for the treatment of AIS patients is not recommended [30]. Oznur Buyu kturan and Mehmet Hanifi Kaya et al to the Cobb angle at 10-30°, Risser AIS patients with values 1-3 for the 6-month Schroth and Lyon method intervention, Found that Schroth practice decreased Cobb angle, improving the Walter Reed Visual Assessment Scale (Walter-Reed Visual Assessment Scale, WRVAS) Points and aspects of ATR of the main lateral bend are more effective, The Lyon (Lyon methods) exercises are more effective than the Schroth exercises in improving the patient’s quality of life. That is, in the short-term treatment, the Lyon method is more effective for the quality of life, while the Schroth exercise method is more effective for body position, spine alignment, and perceived appearance [57].
As shown above, there are many treatments for AIS, and Schroth therapy is effective for AIS, but combined with other methods, comprehensive treatment will be more beneficial. Maharathi, S., Iyengar, A case study by R et al. of a 26-year-old patient with thoracic and lumbar scoliosis that was treated with a biomechanically designed curve correction method. This method corrects pelvic tilt, lumbar abnormality, and thoracic spinal main curvature, advanced to sitting lumbar pelvis combined correction and thoracic spinal main curvature correction; and finally standing lower correction (same sitting position, in two parts). The author of this paper thinks that the sample size is small and the design of others [31]. Monia Lusini, Sabrina Donzelli et al. studied the treatment of patients with lateral cobb>45° and still growing. However, a good brace and good compliance for a total treatment duration of 5 years. The authors of this paper think that time is a flaw [32]. Li Haixia and Wu Jigong et al found that “ in patients with early-onset progressive scoliosis, bracing replacing plaster is mostly effective as a treatment. A small number of ineffective cases require surgery, but at least delay the surgical treatment time and do not limit the chest [33].” Moreover, Hyun Ji Lim, Haesung Yoon, et al. performed the paravertebral muscle elasticity study in patients with AIS correction surgery or brace correction and found that the stiffness of the concave lateral paravertebral muscle was significantly improved in the first 6 months, compared with the effect of the brace group. However, one year later, the paravertebral muscles regained their original appearance and the two treatment groups were not significantly different [34].
For these traditional AIS correction therapies, Stefano Negrini and Silvia Minozzi et al. suggested that bracing has positive implications for controlling the deterioration of curvature. There is now a lack of randomized controlled trials and a low level of evidence. Other designs such as prospective studies need to be adopted and incorporated later. Also, the future focus is on participant outcomes, adverse effects, ways to improve adherence, and the utility of specific scoliosis physiotherapy exercises based on a brace [35].
There is still some controversy about the significance of Schroth therapy in the correction therapy of many AIS. The articles of Vanja Dimitrijevic and Dejan Viduka support that Schroth has more effect on idiopathic scoliosis than core stability training, but both are effective on disease [36]. Chen Yonghuan and Zhang Zhendong et al. disagree that exercise intervention can reduce Cobb angle more than traditional therapy. However, the difference in efficacy between exercise therapies is not significant, and Yoga may be the most effective. Schroth The method effect is ranked in the bottom two of the types explored [37]. Joseph M. Day and Jeremy Fletcher et al. support Chen Yonghuan’s conclusion that both Schroth and SEAS methods effectively improve AIS and Cobb, but SEAS reduces Cobb more than Schroth [38]. Similarly, the Ceballos-Laita,
L. And Carrasco-Uribarren agreed that “Schroth contrast no intervention or other conservative methods” can effectively improve several important efficacy indicators of AIS patients aged 10-18 years, but the Cobb angle reduction is lower than the Minimum Clinical Significance Difference value (MCID), requiring further research on better multi-means synergistic therapy and the medium and long-term efficacy after Schroth intervention [39].
Limitations and challenges of the current study
The effect of the treatment of AIS is controversial: Seung-Min Baika et al. summarized various types of exercise programs to improve postural balance in patients with idiopathic scoliosis and found that the effects of different types of exercise on the balance ability of AIS are still controversial. Interventions to stimulate the postural system, such as hippotherapy, Schroth exercise, PSSE, trunk stabilization, PNF exercise, but geometric and mechanical resistance, such as stretching and self-stretching exercises, did not affect postural balance in AIS patients. The investigators recommend that therapists use exercise therapy to control balance disorders [40]. Similarly, Zapata KA and Sucato DJ et al. also found that the intervention using PSSE (BSPTS) was significantly controlled in patients with mild AIS [41]. Vaiva Seleviciene and Aiste Cesnaviciute et al. mentioned that Schroth is the most studied and effective, but BSPTS and SEAS can stabilize or even reduce the Cobb angle. Of course, only the Schroth method can effectively improve the trunk rotation problem, but the Schroth and SEAS can significantly improve the quality-of-life indicators [19]. Regarding the efficacy question of AIS exercise therapy, Clare Shere and Emma M. Clark Point out the lack of high-quality evidence on the relationship between isolated skeletal muscle overactivity and AIS, and extensive research is needed to reduce confounding factors to explore the role of overexercise skeletal muscle in the pathogenesis of AIS [42].
Similarly, regarding the issue of Schroth combination therapy, Lenaic Minjolleta and Kariman Abelin-Genevois et al compared female patients and peer-healthy people one month after the end of brace treatment, and found that weight and BMI harmed AIS patients. However, there are few studies on this aspect in Schroth research [43].
Xiao Luwei and Gong Lei et al. agree with Schroth and other PSSEs, which can delay or avoid the improvement of the symptoms of support and surgical intervention in AIS patients. However, the research evidence is still insufficient [44].
In addition, Karina Zapata and Eric C. Parent et al. stated ① paying attention to keep the patient in a relaxed position, otherwise, it will overestimate the efficacy of exercise. ② Future exercise studies should be patient guidance at X-ray imaging. ③ Shooting X-rays under correct posture and natural posture-Use EOS imaging to monitor the ability of patients for corrective exercise, understand the relative effects of various correction instructions, and determine the three-dimensional nature of the exercise [10].” This shows that the standard evaluation method in future studies is very important for the evaluation of the efficacy. Indeed, later high-grade research evidence is important to clarify these contradictory findings. Michele Romano and Silvia Minozzi et al argued that” compared with electrical stimulation, traction, and postural training, SSE is more able to avoid the development of scoliosis. However, the level of evidence is insufficient, and more high-quality studies are needed to recommend them to clinical treatment in the future [45].”
Taken together with the above, the challenges of Schroth therapy in treating AIS focus on inconsistency in efficacy, comparison with other therapies, lack of high-quality evidence to support its specific mechanism of action and research methodological limitations. These limitations highlight the need for future studies with more rigorous designs, diverse means of assessment, and larger sample sizes to more accurately define the effectiveness, and scope of Schroth therapy and its role in multimodal treatment strategies.
Future research prospects of Schross therapy in the field of scoliosis prevention and control
Recently, Matthew Jamison and Mark Glover et al. studied lumbar pelvic posture in patients with AIS and found that the anterior angle of the sitting pelvis was smaller than that of normal women, and the posterior angle was greater than their peers. At the same time, healthy women are more likely to stay between 15° and 20° for the short term or duration, and regularly extend, compared with AIS patients [46]. Schroth Method has an impact on the “patient conscious” extension of the lumbar spine-pelvis. And under the sit position to promote the recovery of pelvic forward tilt angle in patients with AIS. In addition, Joseph M. Day and Jeremy Fletcher et al. propose that a set of core measures will better serve patients with AIS. Such effort may not only provide a more effective mechanism for assessing PSSE, but also help clinicians improve the treatment of patients with AIS [38]. The author of this paper also believes that: Schroth, the exercise method can be used to improve a unique version of Risser 4 adults in the future. Since the purpose of this correction method is for patients with severe idiopathic scoliosis, try can improve the movements extend the training time, or increase the frequency to benefit patients with Cobb angle 45°. Men-Jia You and Ze-Yu Lu et al. propose that more randomized controlled trials are needed in the future to verify the effectiveness of PSSE in patients with Cobb angle greater than or equal to 30°. Meanwhile, future RCT studies should consider the impact of different control measures on PSSE efficacy [52].
In addition to the therapeutic goal of AIS, Tuğba Kuru Çolak and Burcin Akcay et al. suggest that it is possible to largely correct curvature and prevent progression from treatment due to appropriate conservative treatment with patients, family members, and clinicians. It is therefore recommended that clinicians and researchers consider these points in the conservative treatment of AIS. Simultaneous comparison of different types of exercises and stents, as well as the duration and intensity of treatment, may be specific topics for future studies [26].
Sanja Schreiber and Daniel Whibley et al. recommend: developing minimum standards for Schroth PSSE trial reporting, including pre-registration of a detailed study protocol, provision of appropriate PSSE labeling, use of Schroth classification system and qualified Schroth therapists, naming and describing specific exercises according to the type of Schroth curve, and provision of treatment dose, prescription method, and compliance. To improve the evidence base of Schroth and provide a good resource for subsequent scientific research reviews [47]. The decline of cardiopulmonary function in AIS patients is one of the symptoms of this chronic disease, but the existing static assessment methods are imperfect [48]. In the future, Schroth methods can be used to improve breathing using the newly proposed dynamic respiratory assessment method, exploring the ability of Schross correction to improve cardiopulmonary function in patients before and after intervention. The same opinion is given by Chen Chenting and Xu Jialu et al. [55] And the comparison of other internationally famous orthopedic methods in cardiopulmonary function can provide a basis for exploring “which exercise therapy is the best”. Schreiber, S. And Eric C. Parent proposed that we can explore which types of children are more likely to benefit from the short-term treatment of Schroth therapy [27]. China has gradually stepped into the elderly society. For elderly patients (older than 65 years old), Schroth exercise therapy will be conducted to explore the effect of IS treatment and determine the possible training methods and training movements.
Conclusion
As one of the most important exercise correction methods for scoliosis worldwide, Schroth fully embodies innovative thinking and patient-centered care concepts. This approach is based on a rational theoretical framework and is implemented through personalized treatment planning. However, the effectiveness of Schroth can coexist with the challenges. The inconsistency in treatment effects, comparison with the effects of other therapies, and the lack of high-quality evidence to clarify its specific mechanism of action highlight the limitations of the current study. In particular, deeper research and more rigorous methodological design are needed in terms of therapy selection, standardization of exercise programs, and how to maximize treatment effects. In addition, although the comparative advantages of Schroth and other conservative therapies and surgical treatments are reflected, more high-quality studies are needed to determine which exercise correction method is optimal.
Future research direction should focus on improving the evidence base of Schroth, including establishing unified treatment effect evaluation criteria, optimizing treatment options to adapt to different severity and age groups, exploring the synergistic mechanism of interaction between Schroth and other therapies, and using innovative technologies such as two-way standing weight full-length imaging system (EOS imaging) to accurately assess corrective effect. In addition, the application of Schroth in specific populations (e.g., elderly populations), the potential impact on cardiopulmonary function, and how to prevent scoliosis progression through exercise therapy are also areas for further discussion. In conclusion, Schroth has shown its potential in the treatment of AIS, but its exact efficacy and optimal way of application still need to be clarified through high-quality scientific studies to guide clinical practice and optimize patient outcomes.
Highlight
Innovative non-surgical approach: The Schroth method is a three-dimensional corrective exercise therapy for Adolescent Idiopathic Scoliosis (AIS), addressing spinal asymmetry, muscle imbalance, and postural dysfunction.
Biomechanical and neuromuscular integration: The method incorporates rotational breathing, sensorimotor training, and neuromuscular re-education to enhance spinal alignment and postural control.
Proven clinical efficacy: Studies confirm that Schroth therapy improves Cobb angle, trunk rotation, and Health-Related Quality of Life (HRQoL), with superior outcomes compared to general physiotherapy.
Synergistic effects with other therapies: Combining Schroth with bracing (e.g., Chêneau, Boston), Pilates, and Electrical Muscle Stimulation (EMS) enhances treatment effectiveness and patient adherence.
Comparison with conservative and surgical treatments: While Schroth outperforms some physiotherapeutic methods (e.g., SEAS, PNF) in correcting AIS, its long-term efficacy relative to bracing and surgery requires further investigation.
Limitations and future directions: Standardized protocols, long-term follow-up, and advanced imaging (e.g., EOS) are essential for refining Schroth therapy’s role in AIS management.
References
- Adolescent idiopathic scoliosis. Nat Rev Dis Primers. 2015; 1: 15063.
- Konieczny MR, Senyurt H, Krauspe R. Epidemiology of adolescent idiopathic scoliosis. J Child Orthop. 2013; 7: 3-9.
- Weiss HR. The method of Katharina Schroth history, principles and current development. Scoliosis. 2011; 6: 17.
- Ren J, Kong L, Wu Z, Zhou X, Huang Q, He T, et al. Benefits on pain and mental health of manual therapy for idiopathic scoliosis: A meta-analysis. Front Endocrinol. 2022; 13: 1038973.
- Bezalel T, Carmeli E, Levi D, Kalichman L. The Effect of Schroth Therapy on Thoracic Kyphotic Curve and Quality of Life in Scheuermann’s Patients: A Randomized Controlled Trial. Asian Spine J. 2019; 13: 490-499.
- Pugacheva N. Corrective exercises in multimodality therapy of idiopathic scoliosis in children analysis of six weeks efficiency pilot study. Stud Health Technol Inform. 2012; 176: 365-371.
- Dimitrijević V, Šćepanović T, Jevtić N, Rašković B, Milankov V, Milosević Z, et al. Application of the Schroth Method in the Treatment of Idiopathic Scoliosis: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2022; 19: 16730.
- Weiss HR, Weiss G, Schaar HJ. Incidence of surgery in conservatively treated patients with scoliosis. Pediatr Rehabil. 2003; 6: 111118.
- Aktan D, Erdoganoglu Y. Effect of short-term 3-dimensional Schroth exercises in adolescent idiopathic scoliosis: An observational study. J Manipulative Physiol Ther. 2021; 44: 612-620.
- Zapata K, Parent EC, Sucato D. Immediate effects of scoliosis-specific corrective exercises on the Cobb angle after one week and after one year of practice. Scoliosis Spinal Disord. 2016; 11: 36.
- Gao A, Li JY, Shao R, Wu TX, Wang YQ, Liu XG, et al. Schroth exercises improve health-related quality of life and radiographic parameters in adolescent idiopathic scoliosis patients. Chin Med J. 2021; 134: 2589-2596.
- Park J, So WY. The Effect of the Schroth Rehabilitation Exercise Program on Spinal and Feet Alignment in Adolescent Patients with Idiopathic Scoliosis: A Pilot Study. Healthcare. 2022; 10: 398.
- Skaggs K, Lin AJ, Andras LM, Illingworth KD, Skaggs DL. Standing in Schroth trained position significantly changes Cobb angle and leg length discrepancy: a pilot study. Spine Deform. 2020; 8: 11851192.
- Karavidas N, Iakovidis P, Chatziprodromidou I, Lytras D, Kasimis K, Kyrkousis A, et al. Physiotherapeutic scoliosis-specific exercises can reduce the risk for progression during early growth in curves below 25°: prospective control study. Eur J Phys Rehabil Med. 2024; 60: 331-339.
- Kuru T, Yeldan İ, Dereli EE, Özdinçler AR, Dikici F, Çolak İ. The efficacy of three-dimensional Schroth exercises in adolescent idiopathic scoliosis: a randomised controlled clinical trial. Clin Rehabil. 2016; 30: 181-190.
- Khan F, Chinnery L, Loveridge J. Can physiotherapy alone reduce spinal curvature in patients with idiopathic scoliosis? Arch Dis Child. 2023; 108: 323-325.
- Fan Y, Ren Q, To MKT, Cheung JPY. Effectiveness of scoliosis-specific exercises for alleviating adolescent idiopathic scoliosis: a systematic review. BMC Musculoskelet Disord. 2020; 21: 495.
- Berdishevsky H, Lebel VA, Bettany-Saltikov J, Rigo M, Lebel A, Hennes A, et al. Physiotherapy scoliosis-specific exercises a comprehensive review of seven major schools. Scoliosis Spinal Disord. 2016; 11: 20.
- Seleviciene V, Cesnaviciute A, Strukcinskiene B, Marcinowicz L, Strazdiene N, Genowska A. Physiotherapeutic scoliosis-specific exercise methodologies used for conservative treatment of adolescent idiopathic scoliosis, and their effectiveness: An extended literature review. Int J Environ Res Public Health. 2022; 19: 9240.
- Bettany-Saltikov J, Parent E, Romano M, Villagrasa M, Negrini S. Physiotherapeutic scoliosis-specific exercises for adolescents with idiopathic scoliosis. Eur J Phys Rehabil Med. 2014; 50: 111-121.
- Xu J, Chen M, Wang X, Xu L, Luo X. Global research hotspots and trends in non-surgical treatment of adolescent idiopathic scoliosis over the past three decades: a bibliometric and visualization study. Front Pediatr. 2024; 11: 1308889.
- Rrecaj-Malaj S, Beqaj S, Krasniqi V, Qorolli M, Tufekcievski A. Outcome of 24 weeks of combined Schroth and Pilates exercises on Cobb angle, trunk rotation, chest expansion, flexibility and quality of life in adolescents with idiopathic scoliosis. Med Sci Monit Basic Res. 2020; 26: e920449.
- Fang MQ, Huang XL, Wang W, Li YA, Xiang GH, Yan GK, et al. The efficacy of Schroth exercises combined with the Chêneau brace for the treatment of adolescent idiopathic scoliosis: a retrospective controlled study. Disabil Rehabil. 2022; 44: 5060-5068.
- Larni Y, Mohsenifar H, Ghandhari H, Salehi R. The effectiveness of Schroth exercises added to the brace on the postural control of adolescents with idiopathic scoliosis: Case series. Ann Med Surg. 2022; 84: 104893.
- Kurak K, Altunhan A, Açak M, Korkmaz MF, Düz S. The Effect of Electrical Muscle Stimulation Enhanced Schroth Method Training on Cobb Angle and Quality of Life in Patients with Scoliosis. Pak J Med Health Sci. 2022.
- Kuru Çolak T, Akçay B, Apti A, Çolak İ. The effectiveness of the Schroth Best Practice Program and Chêneau-type brace treatment in adolescent idiopathic scoliosis: Long-term follow-up evaluation results. Children. 2023; 10: 386.
- Schreiber S, Parent EC, Khodayari Moez E, Hedden DM, Hill DL, Moreau M, et al. Schroth physiotherapeutic scoliosis-specific exercises added to the standard of care lead to better Cobb angle outcomes in adolescents with idiopathic scoliosis: a randomized controlled trial. PLoS One. 2016; 11: e0168746.
- Mohamed N, Acharya V, Schreiber S, Parent EC, Westover L. Effect of adding Schroth physiotherapeutic scoliosis-specific exercises to standard care in adolescents with idiopathic scoliosis on posture assessed using surface topography: a secondary analysis of a randomized controlled trial. PLoS One. 2024; 19: e0302577.
- Shah J, Padma Priya T, Arumugam P, et al. Effect of Schroth method and scientific exercise approach to scoliosis (SEAS) on the Cobb angle among adolescents with idiopathic scoliosis: a comparative study. Ann Rheum Dis. 2019; 78: 2151-2152.
- Mohamed RA, Yousef AM. Impact of Schroth three-dimensional vs proprioceptive neuromuscular facilitation techniques in adolescent idiopathic scoliosis: a randomized controlled study. Eur Rev Med Pharmacol Sci. 2021; 25: 7717-7725.
- Maharathi S, Iyengar R, Chandrasekhar P. Biomechanically designed Curve Specific Corrective Exercise for Adolescent Idiopathic Scoliosis gives significant outcomes in an Adult: A case report. Frontiers in Rehabilitation Sciences. 2023; 4: 1127222.
- Lusini M, Donzelli S, Minnella S, Zaina F, Negrini S. Brace treatment is effective in idiopathic scoliosis over 45°: an observational prospective cohort controlled study. Spine J. 2014; 14: 1951–1956.
- Li H, Wu J, Song L, et al. The efficacy of bracing in the treatment of progressive early-onset scoliosis. Sci Rep. 2024; 14: 10208.
- Lim HJ, Yoon H, Kim J, et al. Comparison of elasticity changes in the paraspinal muscles of adolescent patients with scoliosis treated with surgery and bracing. Sci Rep. 2024; 14: 5623.
- Negrini S, Minozzi S, Bettany-Saltikov J, Chockalingam N, Grivas TB, et al. Braces for idiopathic scoliosis in adolescents. Cochrane Database Syst Rev. 2015; 6: CD006850.
- Dimitrijević V, Viduka D, Šćepanović T, Maksimović N, Giustino V, et al. Effects of Schroth method and core stabilization exercises on idiopathic scoliosis: a systematic review and meta-analysis. Eur Spine J. 2022; 31: 3500–3511.
- Chen Y, Zhang Z, Zhu Q. The effect of an exercise intervention on adolescent idiopathic scoliosis: a network meta-analysis. J Orthop Surg Res. 2023; 18: 655.
- Day JM, Fletcher J, Coghlan M, Ravine T. Review of scoliosis-specific exercise methods used to correct adolescent idiopathic scoliosis. Arch Physiother. 2019; 9: 8.
- Ceballos-Laita L, Carrasco-Uribarren A, Cabanillas-Barea S, PérezGuillén S, Pardos-Aguilella P, et al. The effectiveness of Schroth method in Cobb angle, quality of life and trunk rotation angle in adolescent idiopathic scoliosis: a systematic review and metaanalysis. Eur J Phys Rehabil Med. 2023; 59: 228–236.
- Baik SM, Kim SH, Lee JH. A scoping review of the different types of exercise programs proposed for the improvement of postural balance in adolescents with idiopathic scoliosis. J Back Musculoskelet Rehabil. 2023; 36: 1261–1272.
- Zapata KA, Sucato DJ, Jo CH. Physical Therapy Scoliosis-Specific Exercises may reduce curve progression in mild adolescent idiopathic scoliosis curves. Pediatr Phys Ther. 2019; 31: 280–285.
- Shere C, Clark EM. Systematic review of the association between isolated musculoskeletal hypermobility and adolescent idiopathic scoliosis. Arch Orthop Trauma Surg. 2023; 143: 3055–3076.
- Minjollet L, Abelin-Genevois K, Chelle GD, Sakoun L, Pujol A, et al. Are trunk muscles weaker in adolescent females with adolescent idiopathic scoliosis compared with their healthy counterparts? Iso-kinet Exerc Sci. 2021; 1–9.
- Gong L, Fang L, Ye X, Fan I, Jiang Y, et al. Progress in the treatment of adolescent idiopathic scoliosis in China. 2020; 2: 184–189.
- Romano M, Minozzi S, Zaina F, Saltikov JB, Chockalingam N, et al. Exercises for adolescent idiopathic scoliosis: a Cochrane systematic review. Spine. 2013; 38: E883–E893.
- Jamison M, Glover M, Peterson K, DeGregorio M, King K, et al. Lumbopelvic postural differences in adolescent idiopathic scoliosis: a pilot study. Gait Posture. 2022; 93: 73–77.
- Schreiber S, Whibley D, Somers EC. Schroth physiotherapeutic scoliosis-specific exercise (PSSE) trials: systematic review of methods and recommendations for future research. Children. 2023; 10: 954.
- Wang S. Application of cardiopulmonary exercise test in adolescent patients with scoliosis. Summary of papers of the 13th National Sports Science Conference – Wall Newspaper Exchange (Sports Medicine Branch). 2023; 2: 95–97.
- Thompson JY, Williamson EM, Williams MA, Heine PJ, Lamb SE, et al. Effectiveness of scoliosis-specific exercises for adolescent idiopathic scoliosis compared with other non-surgical interventions: a systematic review and meta-analysis. Physiotherapy. 2019; 105: 214–234.
- Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, et al. 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018; 13: 3.
- Day JM, Fletcher J, Coghlan M, Ravine T. Review of scoliosis-specific exercise methods used to correct adolescent idiopathic scoliosis. Arch Physiother. 2019; 9: 8.
- You MJ, Lu ZY, Xu QY, Chen PB, Li B, et al. Effectiveness of physiotherapeutic scoliosis-specific exercises on 3-dimensional spinal deformities in patients with adolescent idiopathic scoliosis: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2024; In press.
- Motion PT Group. Schroth method of scoliosis treatment in physical therapy. Website article. 2023.
- Dimitrijević V, Šćepanović T, Jevtić N, Rašković B, Milankov V, et al. Application of the Schroth Method in the treatment of idiopathic scoliosis: a systematic review and meta-analysis. Int J Environ Res Public Health. 2022; 19: 16730.
- Chen C, Xu J, Li H. Effects of Schroth 3D exercise on adolescent idiopathic scoliosis: a systematic review and meta-analysis. Children. 2024; 11: 806.
- Baumann AN, Orellana K, Oleson CJ, Curtis DP, Cahill P, et al. The impact of patient scoliosis-specific exercises for adolescent idiopathic scoliosis: a systematic review and meta-analysis of randomized controlled trials with subgroup analysis using observational studies. Spine Deform. 2024; 12: 545–559.
- Büyükturan Ö, Kaya MH, Alkan H, Büyükturan B, Erbahçeci F. Comparison of the efficacy of Schroth and Lyon exercise treatment techniques in adolescent idiopathic scoliosis: a randomized controlled, assessor and statistician blinded study. Musculoskelet Sci Pract. 2024; 72: 102952.